From The Conversation…
Have you ever wondered why, in most species, males are larger and more ornamented than females? It’s an evolutionarily determined aspect of biology, but what does it mean for human health and disease? What are the implications of needing one chart to describe normal growth in boys, and another to describe normal growth in girls? Why are there two normals for growth, and does it matter for a disease of growth like cancer?
I’m a pediatric brain tumor doctor and scientist and am interested in developing new treatments for glioblastoma (GBM) and other malignant brain tumors. Glioblastoma is the most common malignant brain tumor and killed the late Sens. John McCain and Ted Kennedy, and Beau Biden III, the eldest child of former U.S. Vice President Joe Biden.
In this new year, about 22,000 Americans will develop glioblastoma, and nearly the same number will die from it. While GBM occurs in both males and females, we can reliably predict that of the 22,000 new cases, 8,500 will be in females while the remaining 13,500 cases will be in males. Moreover, the female GBM patients can be expected to survive about six months longer than the male patients, on average.
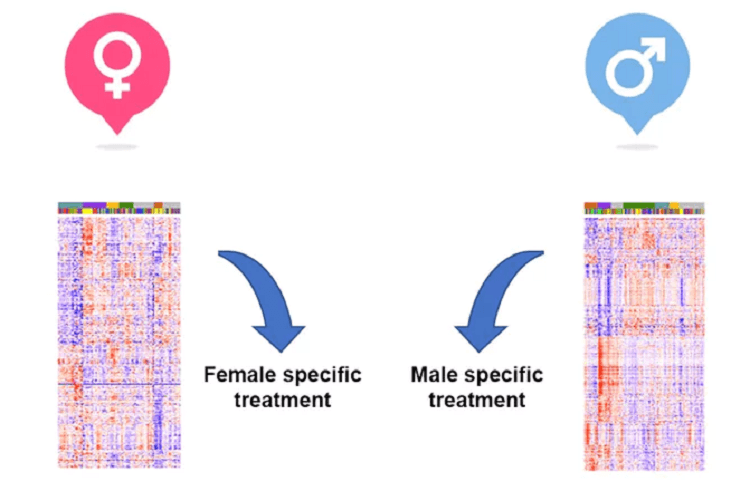
My colleagues and I wondered whether basic differences in biology might explain why males were more vulnerable to these malignant brain tumors and why their survival time was shorter than for females. We hypothesized that if there were differences between the male and female version of glioblastoma, we might be able to generate new, sex-specific approaches to treatment that would improve outcomes for everyone.
Sex and disease
Many human diseases exhibit substantial sex differences in their frequency and severity. Autoimmune disorders such as systemic lupus erythematosus occur nine times more frequently in females than males, and psychiatric diseases such as like depression occur nearly twice as frequently in females compared to males. The implications of sex differences in cancer have not been extensively investigated in clinical or laboratory research.
While there is a great interest in developing more personalized approaches to cancer treatment, a patient’s sex, a key feature of personalization, has not yet been incorporated into this paradigm. In our recent study in Science Translational Medicine, my collaborators and I provide what we think is compelling evidence that patients’ sex should be incorporated into treatments for glioblastoma and more thoroughly investigated in the laboratory.